













The Value Journey: Improving Cost Structure Through Performance Improvement
The Value Journey: Improving Cost Structure Through Performance Improvement
Feature: Victor G. DeMarco, CPA, Barton S. Richards, MBA, CHFP, Larry Volkmar, RN, BSN, MBA, FACHE, and Lauren C. Gorski, MBA, MHSM
A New York hospital offers a case example of how to undertake performance improvement on a systemwide scale to prepare for value-based care.
In 2012, Bronx-Lebanon Hospital Center in New York began preparing for the shift to a value-based payment system by performing a complete review of its operations. This internal organizational review provided the organization’s senior executives with clear evidence that the hospital was operating efficiently, in both fixed and variable cost structures. Despite the apparent strength of the organization in its current state, however, the senior executives acknowledged that the emerging value-based healthcare environment would present new complexities that would challenge the organization’s ability to maintain financial stability in the future. They therefore undertook an initiative to verify the organization’s current operational efficiencies and explore new cost-saving opportunities.
Bronx-Lebanon Hospital Center is the largest not-for-profit health system serving the South and Central Bronx, with 972 beds at two major hospital divisions, comprehensive psychiatric and chemical dependency programs, two specialized long-term care facilities, and an extensive BronxCare Network of practices that provides more than 1 million outpatient visits annually. Its emergency department (ED) also sees about 141,000 visits annually, making it among the busiest in New York. It serves a patient population with high disease incidence rates, large numbers of minorities and immigrants, and low socioeconomic status. Much of the South Bronx is also designated as a medically underserved and health professional shortage area.
This initiative was conducted in two separate phases to identify savings and efficiency opportunities. The first phase involved an in-depth assessment of variable costs, such as supplies and contracted services, and the second phase focused on employee and provider productivity.
Once savings and efficiency opportunities were identified, it was decided that changes should be implemented immediately to stay ahead of the changing healthcare landscape. By 2015, improvement opportunities identified and implemented as a result of the initiative amounted to $20 million in cost savings and operational efficiencies. What follows is an account of how Bronx-Lebanon was able to achieve these results.
Uncovering and Implementing Nonlabor Cost Savings Opportunities
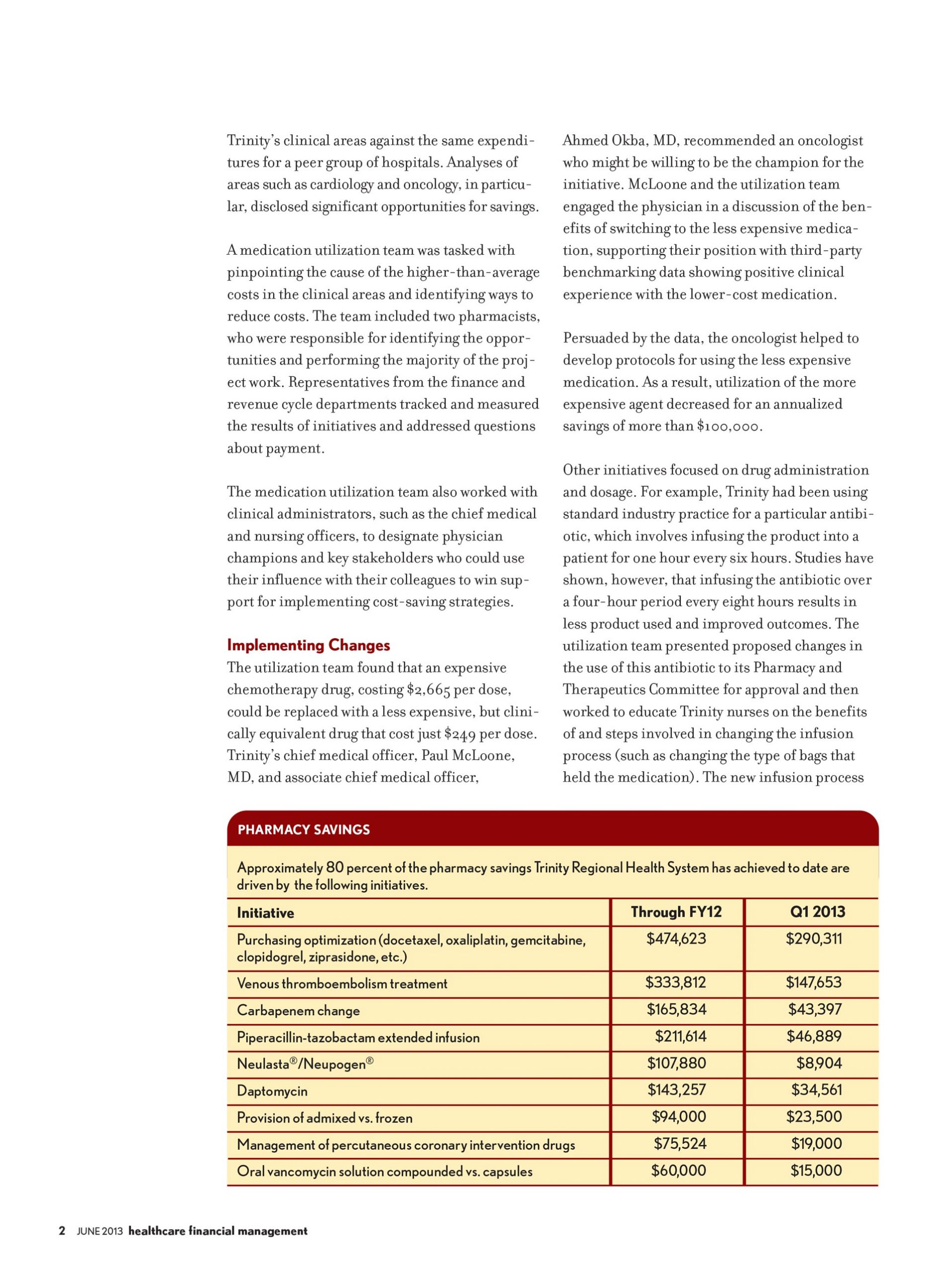
During the first phase of the project, each department’s variable-cost structure was analyzed for areas of opportunity. Focus teams, which included an executive sponsor and the department director or manager, were created for each initiative. The teams were tasked with identifying areas of cost savings and efficiency opportunities in each department, looking at everything from supply costs to clinical practices to services contracts. As a result, major initiatives were undertaken in areas such as the pharmacy, medical-surgical supplies, contracted services, employee benefits, support services, and the laboratory. The following discussion focuses on four of these areas.
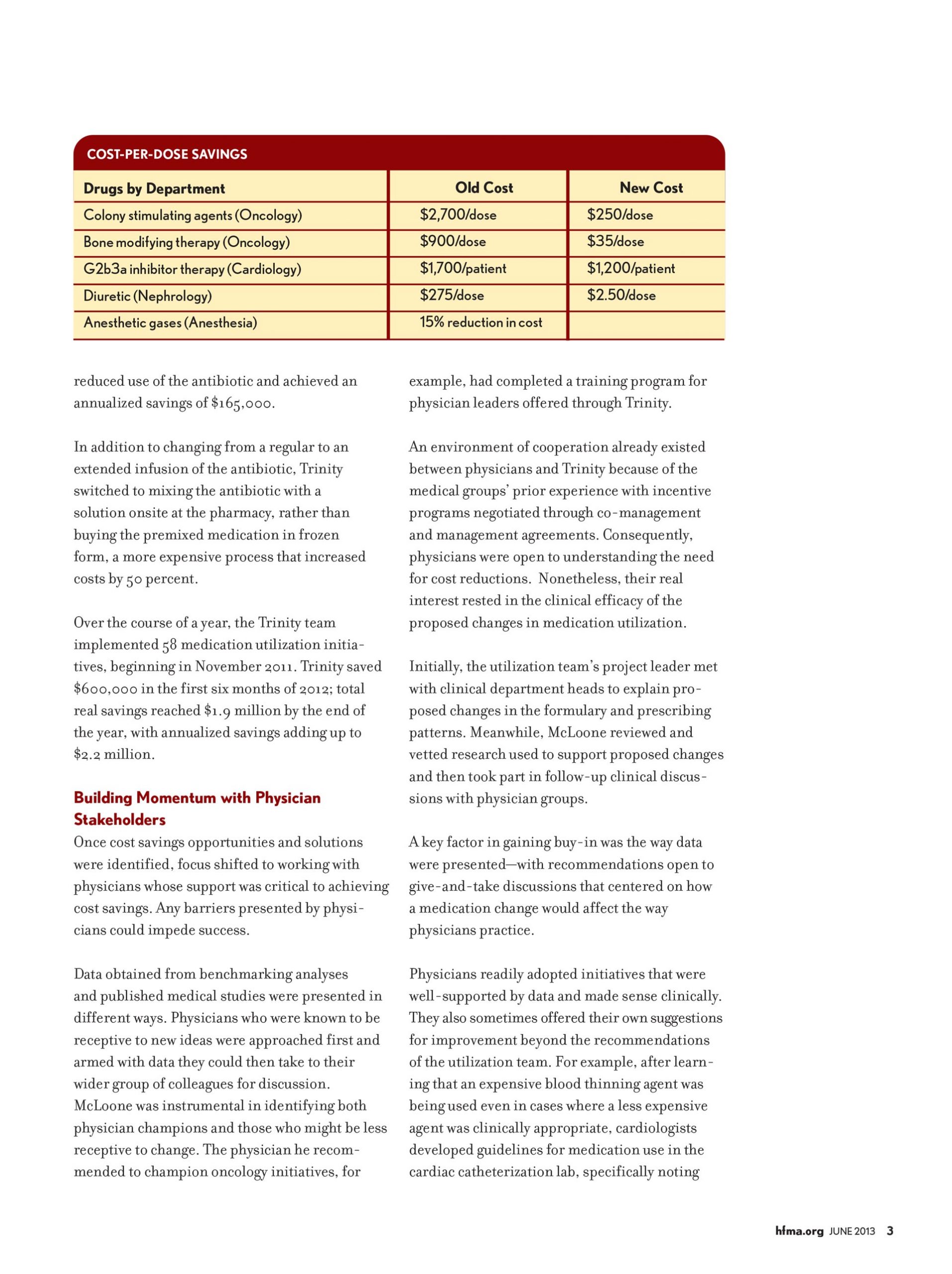
Pharmacy. The focus team charged with improving pharmacy performance achieved notable success using a process that began with a thorough assessment of pharmacy operations. This assessment included an in-depth review of the department’s policies and procedures, purchase orders, chargemaster, and usage data. The team also was able to formulate conclusions by observing the pharmacy’s day-to-day processes and interactions with clinical staff, including models of care, operations, cost-reduction opportunities, drug distribution, inventory reduction, and physician relations. As a result of reviewing the usage data, the team recommended that therapeutic substitutions of clinically equivalent pharmacy products be made, including in the areas of proton pump inhibitors and cervical ripening agents. Support for these changes was bolstered through education aimed at raising awareness by the clinical staff, and adjustments were made to the hospital’s formulary.
As a result of this assessment, the focus team undertook three primary initiatives involving collaboration with pharmacy, clinical, regulatory, and finance staff.
First, to better serve the needs of the community, Bronx-Lebanon partnered with a local retail pharmacy to address the needs of the hospital’s patient population, particularly with respect to home prescription delivery and payment options. This initiative sought to improve medication adherence in the hospital’s low-income population, thereby helping to reduce readmissions and redirect patients from the emergency department (ED) to an outpatient practice.
Second, Bronx-Lebanon worked with the lead physician to develop a program that would address the needs of patients who were directed to receive injectable medications for multiple sclerosis. The program brought injectable drug preparation and the infusion process in-house, ensuring that patients were kept consistently under the care of their existing provider. This change also resulted in the creation of a new revenue stream.
Third, the team facilitated collaboration between pharmacy and clinical staff on an educational initiative aimed at reducing utilization of certain high-cost drugs by raising physician awareness of clinically equivalent substitutes and utilization guidelines. By working with a physician leader from the hospital and utilizing third-party clinical experts, the team was able to increase physician participation. Committee meetings and educational sessions were held on a regular basis to keep clinical leadership apprised of changes and include them in the decision-making process.
Together, these pharmacy-focused initiatives enabled Bronx-Lebanon to improve Healthcare Effectiveness Data and Information Set (HEDIS) and pay-for-performance measures and keep the pharmacy on track to meet its budget.
Medical-surgical supplies. Another focus team was able to realize significant savings through an operating room (OR) inventory project. In partnering with materials management and OR personnel, the team performed a complete assessment of the current OR medical-surgical supply inventory. The assessment included reviews of supply usage data, purchase orders, and on-hand inventory data. The team developed a system that allocated inventory into four categories:
- Obsolete (not used or purchased in 12 months)
- Excess (greater than a year’s supply on hand)
- Slow moving (greater than three months’ supply on hand)
- Active
This process allowed the team to focus first on eliminating obsolete and excess inventory before undertaking a complete redesign of the OR storage room and processes. The process provided the groundwork for installing storage equipment and implementing a categorized, cataloged system designed to achieve efficiencies, with PAR levels (i.e., minimum quantities stocked before products would automatically be reordered) set for each inventory item. The team also worked with the surgeons to identify their product preferences, and the variety of products was reduced. Slow-moving and obsolete inventory also were eliminated.
The laboratory. The focus team charged with improving performance in the laboratory also demonstrated how a collaborative approach could produce a positive impact on the hospital’s variable-cost structure. The team not only was able to negotiate better pricing on contracts in areas where there was clearly increased usage, such as the blood and reference lab, but also was able to achieve similar results in other areas where the opportunities were not so clear. Specifically, the team analyzed reagent supplies and testing equipment for usage and effects on productivity through observation and data analysis, and was able to identify significant opportunities in these areas, including the optimization of Bronx-Lebanon’s group purchasing contracts to obtain better pricing on reagent supplies and the acquisition of new equipment that would improve labor productivity. This new equipment required less staff time to operate than the equipment that had been in use.
Support services. The performance improvement efforts that focused on support services, such as biomedical maintenance, dietary, and linen, achieved significant results. The hospital had been using outsourced providers in these areas.
The team considered the total cost elements involved and the micro-economic drivers as part of its effort to analyze costs associated with each service. The team also sought to understand which cost levers to pull and the impact any change would have on overall quality and costs. In the area of food and nutrition, for example, improved quality, make-fresh-versus-buy options, labor inputs, retail pricing, and nursing unit food PAR levels should be considered when undertaking a performance improvement initiative.
Ultimately, the team decided to expand the scope of the biomedical maintenance contract to take over additional equipment, shifting the risk from Bronx-Lebanon to the service provider. Utilization changes were made based on the review of dietary services data to reduce the hospital’s waste. Again, the leadership for these areas was vital in achieving optimum results, with hospital leadership taking on a pivotal role in ensuring that changes were implemented in a timely manner, with appropriate communication to staff and stakeholders, negotiations with suppliers, and changes to processes.
In the nonlabor areas, Bronx-Lebanon’s approach of managing multiple initiatives across its organization resulted in upgraded processes with improved efficiencies, ultimately producing a substantial positive impact on the hospital’s financial performance. The key to success was maintaining a coordinated effort driven by the organization’s major stakeholders. Bronx-Lebanon’s senior management and administrative team were deeply involved throughout the nonlabor phase of the project, holding biweekly steering committee meetings in addition to frequent sub-committee meetings to ensure that the focus areas were continually moving forward. Focus team leaders assumed responsibility for driving cost savings within their respective areas and played an active role in supplier negotiations. Finance staff played an important role in each initiative as well, monitoring progress and providing the project teams with updates including savings impacts to date and quality results. The coordinated effort and buy-in at all levels of the organization resulted in a successful phase of the project.
Uncovering and Implementing Labor Productivity and Efficiency Opportunities
Prior to the start of the project, Bronx-Lebanon maintained an aggressive vacancy control process, concentrating on limiting the amount of contracted resources. With upwards of 4,000 employees, including over 400 salaried physicians, the hospital faced challenges in maintaining consistency and productivity across different locations and service lines.
Under the oversight of Bronx-Lebanon’s senior management, productivity analyses were conducted, focusing on the roles most prevalent across the organization, such as registrars and managers. Staffing productivity savings were identified through benchmarking and volume trend analyses.
In-depth analyses of each service line’s functionality were performed to assess margin contribution. To start, all direct and indirect costs were analyzed, including volume trends over time compared with staffing. Revenues were then assessed to determine the feasibility of sustaining service lines.
A proportional span-of-control review also was performed, which involved identifying staff-to-executive ratios across all areas of the organization. Close attention was given to positions with minimal reporting relationships at the manager and director level. In looking at each department, opportunities to consolidate oversight were considered and staffing adjustments were made to contribute to a flatter staff-to-executive ratio. Through this process, the team identified redundant programs and departmental activities that could be consolidated.
Streamlining the span of control and combining responsibilities enabled the organization to achieve productivity savings. Physician champions for each service line became pivotal in identifying how specific areas could function with optimal staffing during each part of the day.
For example, the chairman of family medicine implemented new processes throughout his department based on an analysis of the data that allowed for the consolidation of responsibilities and the implementation of increased efficiencies, thereby significantly improving productivity.
Such changes were implemented in phases, starting with administrative staff roles and proceeding through clinical roles, and team leaders worked within their respective divisions to maintain systemwide standards for education and goal awareness.
The most challenging piece of the project was the analysis of physician productivity. For each physician, a provider productivity analysis was completed by location and specialty, including patient visit trends, revenue generation, and total compensation. Each physician’s performance was then benchmarked against national standards, and targets for visits by provider on an outpatient basis were identified.
The analysis took into account each physician’s specific role as an important consideration. Many physicians had unique roles, serving in various instances as chairmen, division chiefs, or medical educators for residents. To reach optimal productivity with its physicians, Bronx-Lebanon is considering a broad range of recommendations, including dedicated inpatient hospitalist and ancillary service models.
Results
Through both the nonlabor and labor phases of its performance improvement project, Bronx-Lebanon was able to achieve more than $20 million in total benefits. The 12-month initial, nonlabor phase of the project yielded savings of more than $5 million in pharmacy initiatives and an additional $6 million from reductions in variable costs, including human resources, ancillary services, support services, purchased services inventory, and supply expenses. The five-month second phase of the project, focusing on labor, achieved $9 million in productivity increases, including $4 million for physicians, $2 million for management and support personnel, $1 million for nonphysician providers, and an additional $2 million in other areas.
Bronx-Lebanon’s improved operational efficiencies have moved the organization closer to becoming a value-based health system and provided a basis for its future continuous growth. The hospital also has recently been selected by the New York State Department of Health as a performing provider system lead for the state’s Delivery System Reform Incentive Payment program, providing the hospital with an additional opportunity for healthcare performance improvement.
Success Factors and Lessons Learned
Performance improvement is an ongoing effort. Based on their experience with Bronx-Lebanon’s comprehensive performance improvement project, the hospital’s senior executives cite three key lessons that they regard as being critical to any such project’s success.
First, the initiatives must be visible throughout the organization, with their importance clearly highlighted and communicated so they are apparent to all staff.
Second, buy-in and staff participation are required, and senior leadership must play an active role in implementation. When new efficiencies are discovered through collaborative efforts such as those that characterize Bronx-Lebanon’s initiative, senior executives should be prepared to move quickly in advancing these changes and improvements to the organization.
Third, performance improvement initiatives can be effectively identified and implemented only through such a collaborative, structured approach, which should be reinforced through ongoing project governance at the senior-leadership level.
On a more specific level, five keys to success can be gleaned from Bronx-Lebanon’s experience:
- Collaboration with physician leaders across service lines, providing strongly data-based support for their decision making
- Inclusion on project teams of individuals who have a familiarity with leading practice models that can be implemented within a short time frame
- Team leadership by individuals who have sufficient communication skills to clarify complex issues for management, thereby promoting expeditious decision making
- Thoroughness in communications aimed at overcoming resistance to change, including educational sessions, one-on-one meetings, regular status updates, and formal steering committee meetings
Strong sponsorship by senior leadership, particularly with regard to labor productivity.
Victor G. DeMarco, CPA, is senior vice president and CFO, Bronx-Lebanon Hospital Center, Bronx, New York, and a member of HFMA’s Metropolitan New York Chapter.
Barton S. Richards, MBA, CHFP, is managing director, The Claro Group, Chicago, and a member of HFMA’s First Illinois Chapter.
Larry Volkmar, RN, BSN, MBA, FACHE, is managing partner, The Claro Group, Chicago.
Lauren C. Gorski, MBA, MHSM, is manager, The Claro Group, Chicago, and a member of HFMA’s First Illinois Chapter.
Publication Date: Wednesday, June 01, 2016